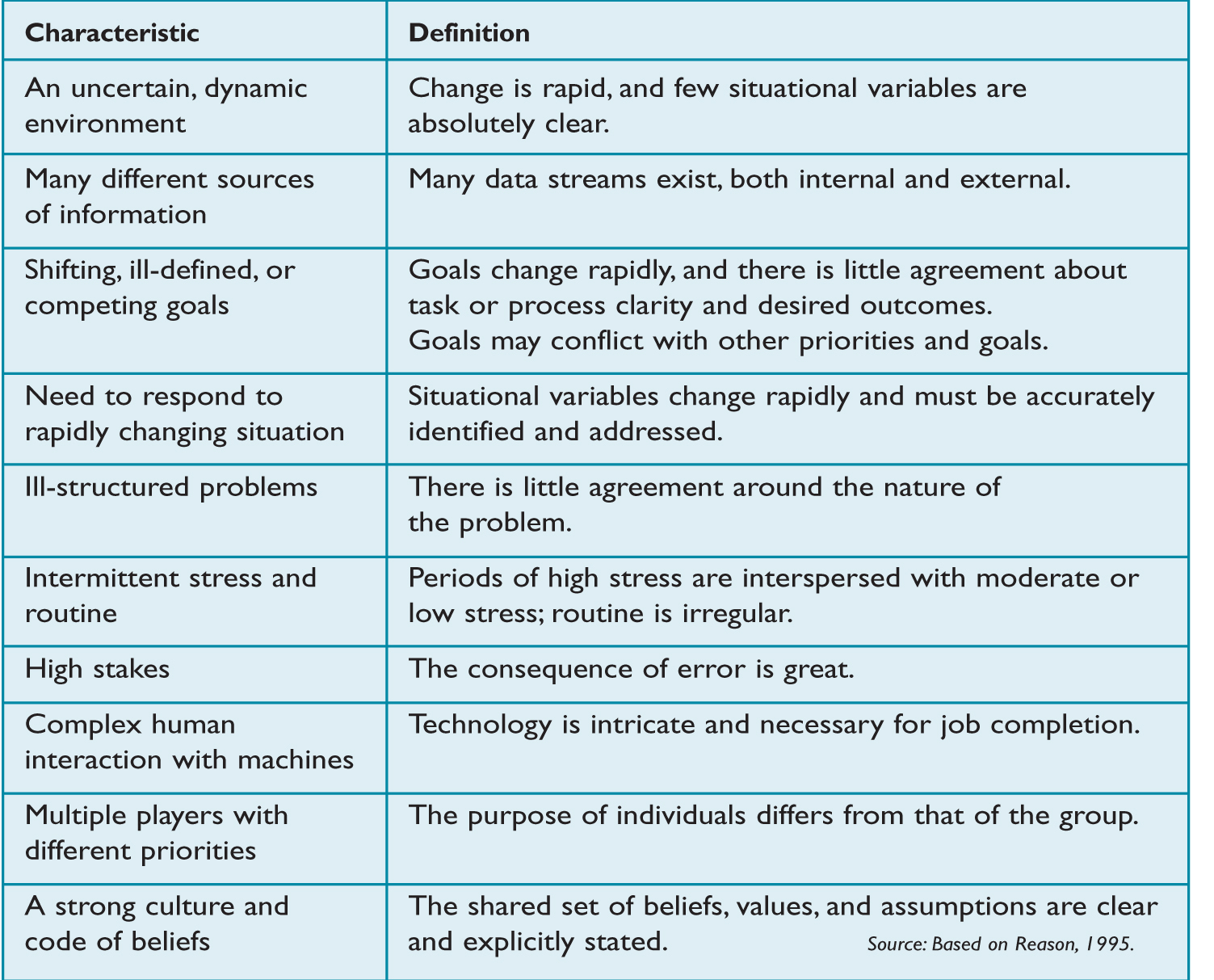
The information-intensive, complex, and dynamic world presents unique challenges for leaders. Never before has information been so available but knowledge been so difficult to create. The Economist (2010) calls this situation the world of “big data” and the consequence a resulting “data exhaustion.” The world of big data isn’t the only element challenging leaders. “Characteristics of a Complex Leadership Environment” provides a quick list of the demands faced by today’s leader, based on the work of James Reason (1995), a scholar who studies learning and failure in high-risk situations. Along the same lines, a study sponsored by the American Management Association in 2007 reported that 82 percent of organizations surveyed thought the pace of change had increased in the previous five years and that at least one major disruptive change had occurred that had affected their organization in the last year.
In the world of big data and high-stakes, disruptive change, learning becomes essential for leadership. Reason may have been concerned with high-risk leadership situations, but he could have easily been referring to any leader. In fact, contemporary leaders in business organizations share many of the same challenges faced by well-known high-stress and high-consequence positions such as pilots, surgery teams, and military quick reaction forces.
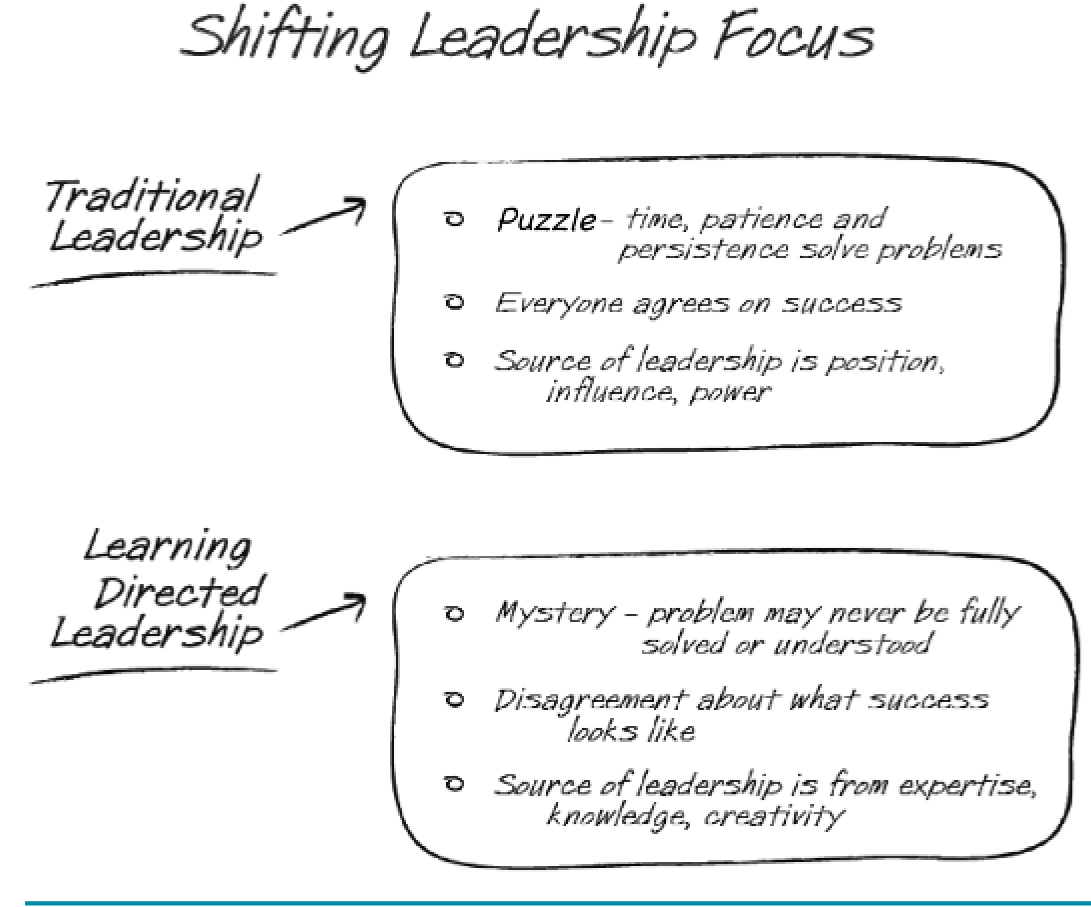
The Shift from Traditional to Learning-Directed Leadership
Traditional approaches to leadership focus on power, influence, and position as the sources of leadership. No doubt, these are important factors. However, they prove less important in a complex and dynamic world where disruptive change is considered normal. Leaders working in the world of “big data” engage learning rather than power, knowledge rather than influence, expertise rather than position. Learning-directed leaders see continual learning, not the hoarding of power and resources, as their primary advantage. At their core, learning-directed leaders work to be open to new information and ready to revise past assessments of a situation, cultivating knowledge, learning, and expertise along the way as described by psychologist Theodore Mills (1967).
Leadership requires a shift in understanding about the nature of problems and how these problems are solved. The study of knowledge distinguishes between ill-structured and well-structured problems. Well-structured problems require time, patience, and persistence. Given enough time and resources, leaders can always solve well-structured problems. An example of a well-structured problem is reducing a budget by 15 percent. On the other hand, determining a new strategic direction in a fast-changing marketplace is an ill-structured problem.
Well-structured problems are the work of traditional leaders. Learning-directed leaders, on the other hand, work to solve ill-structured problems. No matter how much time, persistence, and patience a leader puts into solving an ill-structured problem, it can never be fully understood, and people will never fully agree on one right decision. In fact, there is no single best solution for an ill-structured problem. “Moving from Traditional to Learning-Directed Leadership” represents the shift in thinking required for a leader to be successful in this context. The shift, although difficult, is essential for leading, as an example from the medical profession illustrates.
CHARACTERISTICS OF A COMPLEX LEADERSHIP ENVIRONMENT
Eliminating Infections in Critical Care Medicine
Medical personnel insert or replace thousands of central line catheters each day. These catheters, which are inserted into veins in the neck, groin, or chest, dispense medications or fluids and can be used to measure blood volume. In the most trying cases, a central line catheter can save a life or limit pain. Inserting one of these devices is a common procedure. Unfortunately every year, an estimated 80,000 patients contract an infection that could have been avoided. Between 30,000 and 50,000 of these patients die as a result (Landro, 2010).
The procedures involved in changing a central line catheter may seem simple and routine, but learning to do something other than the existing procedures is much more difficult. In reality, improving the process of inserting or changing central line catheters has proven particularly challenging. Changing a well-established procedure involves monitoring hundreds of pieces of information, coordinating complex processes, and overcoming deeply ingrained cultural barriers.
MOVING FROM TRADITIONAL TO LEARNING-DIRECTED LEADERSHIP
Several factors contribute to the problem. A medical professional may care for hundreds of patients a month. The human mind is only capable of remembering a limited amount of data at any one time and so keeping track of each procedure becomes difficult. Further, many professionals don’t have direct access to the correct supplies. Changing a catheter may prove a challenge because resources come from different locations and quality is difficult to assess. Adding to the problem, changing and inserting a catheter requires coordination among various professionals.
A group of physicians sought to change the way medical professionals go about inserting and changing catheters in patients to decrease the high rate of infection and death. Led by Dr. Peter Pronovost of the Department of Anesthesiology and Critical Care Medicine at the Johns Hopkins Hospital, they tackled the problem by turning learning into action (Pronovost & Vohr, 2010). They began by reviewing prior research on catheter-related infections and related topics. From this research, they identified five practices that showed promise in limiting infection.
First, they introduced an educational program to teach physicians, residents, nurses, and other medical professionals about the existing procedures and how small changes might reduce infections. Second, they created a central cart that included all the materials needed to conduct the procedure with a greater degree of safety. In the past, medical personnel might have to search for the proper equipment, losing valuable time and focus in the process. Third, they instituted a daily care plan meeting that addressed whether patients needed a new catheter. Fourth, and most important, they implemented a checklist procedure, adopted from preflight checklists used by airline flight crews. The process, led by the bedside nurse, ensured that personnel followed proper and safe procedures. The checklist was to be used each time a new catheter was inserted or rewired. Fifth, they called on nurses to stop the process if any care provider failed to follow the guidelines as stated on the checklist. The steps on the checklist were clear and concise. When inserting a catheter, the professionals were to wash their hands; clean the patient’s skin with a disinfectant; wear a cap and gown and use a surgical drape; insert the catheter through parts of the body other than the groin; and remove any unnecessary catheters.
The physicians achieved a successful result by almost any measure. Researchers estimated that, when adopted in 50 intensive care units in Michigan, the procedure might have prevented 2,000 infections, reaching an infection rate of near zero (Landro, 2010). The procedures demonstrate the power of learning-directed leadership. Learning-directed leadership impacts organizational effectiveness through five processes: increasing awareness of a problem or system, learning from (rather than simply repeating) experience, facilitating behavioral change through coordination, improving judgment of individual employees, and breaking down hierarchy to transfer knowledge across levels of the organization. We present each of these in turn.
Increasing Awareness. Like most successful organization-wide learning initiatives, the catheter safety effort began by focusing attention on the general problem. The hospitals that adopted the catheter safety process implemented a training course for the general population and garnered the support of management. Frontline employees, those who were responsible for insertion and replacement of catheters, received additional training that focused on the specific elements of the problem. Increasing awareness stands as the first step in learning by focusing the attention of the entire organization on an otherwise misunderstood or overlooked problem.
Learning from Past Experience. One reason that the intervention proved so successful was that it relied on a comprehensive review of existing knowledge. The researchers didn’t start from scratch; they sifted through years of studies, in fields from medicine to flight crew operations. They identified ways to put these research findings into action. But they went further by culling best practices. They identified what practices were cursory and which were central to success. Much of the success could be attributed to the fact that these techniques had been used before, and only the most successful processes were adopted.
The researchers went beyond use of existing experience; they made gains in applying the model to a new situation. No one could logically accept that a flight crew checklist would be appropriate for a hospital. The researchers knew they had to adapt the checklist for their own unique purposes. The process of adaptation cannot be underestimated, for it seems that many best practices go unused because organizations fail to adapt them to the specific circumstances they face.
Facilitating Behavior Change. The central line catheter awareness program also involved behavioral change by encouraging medical professionals to consider small changes in how they work. Behavioral components included adoption of a common cart, institution of a checklist to detail critical procedures, and establishment of standardized review procedures for each patient.
These changes help medical professionals focus on the processes most important to achieving the goal, in this case infection-free catheter insertion. At the same time, the professionals develop a clearer picture of the larger task, seeing how their individual actions fit into the larger treatment plan for the patient. Learning occurs through the constant monitoring of patient treatment as given by other caregivers. Thus, this approach engages the best element of goal setting. It helps to simplify a complex process by focusing attention on key aspects of a task while simultaneously allowing for learning about the implications for the larger task. The most important behavioral change may not be the actual medical procedures itself, but the improved coordination that results.
We know that learning involves collective rather than just individual processes. Yet, the role of coordination in learning is often characterized as mysterious and therefore often overlooked. Perhaps this is because coordination can be difficult to observe and capture. Psychologist Daniel Wegner (Wegner and Wegner, 1985) has taken some of the mystery out of coordinated learning with something he calls “transactive memory.” His early research was largely confined to laboratory studies. In one study, pairs of individuals who had been in a relationship more than three months were better able to recall words than those who were not in these relationships. Over the last few years, the notion of transactive memory has been confirmed in dozens of studies in real-world settings. These studies largely confirm Wegner’s findings – teamwork matters. The catheter safety program demonstrates the role of transactive memory in learning. Teams that demonstrate transactive memory share three characteristics.
First, team members believe in the credibility of the information shared by other members. The catheter safety program appears to increase credibility because it provides a shared template, common repository, and agreed-upon procedure for documenting knowledge. Essentially, the shared checklist replaces individual memory with a team memory. Credibility increases because the checklist serves as a shared and likely more credible source of memory, so that memory is no longer assigned to the more fallible process of individual cognition.
Second, transactive memory involves effectively coordinating actions. Coordination means that information moves across and between individuals in a way that contributes to the team’s overall performance. The catheter safety program encourages coordination by helping teams establish a common set of procedures that guide action. The development, implementation, and integration of a checklist fosters learning because coordination becomes an everyday practice, not an abstraction. Coordination leads to learning because it necessitates an agreed-upon procedure, standardizes routine processes, and creates a template for improving processes.
Third, the common checklist improves coordination among a group of specialized professionals. Organizations manage complexity by distributing labor. Nurses, physicians, and residents each perform a specific duty. This division of labor helps the organization but creates challenges for coordination. Learning occurs when team members understand, respect, and utilize the unique expertise of these diverse roles. The catheter safety program provides evidence that when learning becomes a daily practice, it improves performance.
Improving Judgment. In addition to creating awareness and making incremental changes to behavior, lessons from catheter safety checklists point to the importance of improving professional judgment. The checklist implementation process marks an important shift from institutionalizing organization-wide policies to allowing experienced professionals to exercise judgment. For example, the development and implementation of a checklist is not abstract but part of the daily routine of professionals. For sure, implementation requires a coordinated effort at all levels of the organization, including strong support from management, but ultimately, the change occurs at the most direct levels of patient care, not policy. The program success results from the learning that occurs as professionals exercise autonomy and judgment unencumbered by overly burdensome institutional rules.
Improving professional judgment is an important part of learning. In a 1986 study, Vimla Patel and colleagues found that experienced physicians saw medical situations in a more holistic and complete way than did residents. In other words, physicians relied on a greater source of data, including patient histories and lifestyle data, to make a diagnosis. In non-routine cases, experts rely on “flexible reasoning” to generate alternatives, revise hypotheses, and develop meaningful courses of action. Judgment and its cousin learning require adapting, looking at a broad range of information, challenging, and understanding context.
Breaking Down Hierarchy. The cornerstone of the catheter safety program can be found in the introduction and use of a common checklist. However, from a learning standpoint, the checklist itself serves simply to facilitate a larger psychological purpose. It facilitates the breakdown of traditional organizational and professional hierarchies.
Medicine’s adoption of checklists builds on a legacy established by commercial pilots. Studies of numerous air tragedies and near misses have revealed that all too often, dysfunctional power dynamics among the flight crews contributed to the disaster. Overly authoritarian cockpit captains ignored the insights and warnings of copilots, leading to a crash or near miss. The checklist serves to neutralize traditional forms of power such as rank or profession because authority no longer rests in the rank of individuals but in their knowledge, and this paves the way for learning. Nurses and residents gain the authority to stop a procedure if it doesn’t conform to guidelines.
Each of these five processes underscores the importance of learning in improving organizational effectiveness. The initial experiment for catheter safety has been adopted by other hospitals around the US. It stands as a remarkable example of learning in organizations. We can’t emphasize enough that the learning from such an effort occurs on two levels. The first level is the learning that occurs from engaging in the process of building the procedure. The second level of learning occurs as an outcome of the continued engagement in the process itself.
A successful program can tell us something important, but an overt collapse of learning can tell us something else. Next we turn to the case of Lehman Brothers and the failure to learn.
Failure to Learn at Lehman Brothers
As one way to understand just how the catheter safety program invokes learning, we can contrast it with an organization that failed to learn. Lehman Brothers can be described as a collapse of learning because it had, at the time of this writing, the largest bankruptcy in the world’s history, topping an estimated $639 billion in assets.
Over years, Lehman grew into a rigid culture, where it enforced strict informal rules for behavior. The culture served the company well at times, but the same rigidity also restricted its ability to learn and adapt. During the mortgage crisis of 2007, the managers at Lehman needed to assess and change their behavior and respond to the need for new direction. Rather, as former chief talent officer Hope Greenfield indicated in Leader to Leader, managers “stood in the sidelines waiting to see who was going to take the reins next” and occupied themselves with “finger pointing and blame.” The culture did not change behaviors even when the company needed that change to survive.
Lehman found itself plagued by widespread turnover, which resulted in continual loss of talent. These trends meant that professional judgment was constantly under threat. As Greenfield pointed out, managers who tried to exercise their professionalism found themselves sidelined and ostracized, and many eventually left the organization. As a result, the culture at Lehman restricted independent professional judgment in favor of rigid thinking. Learning ultimately became stifled.
Team coordination, another hallmark of learning, is built on a foundation of credibility that allows individual team members the freedom to act. However, in cultures that breed a strong sense of competitiveness among managers, it is difficult to build credible, trustworthy teams in which members place the team’s interests and welfare above their personal interests. In this “underdog eat underdog world,” managers prided themselves on their work ethic and fierce competitive spirit rather than good leadership.
This competitive spirit often overshadowed level-headed thinking. The head of Lehmann was bound for retirement, and his number two in command was not a likely successor. This dynamic enhanced the spirit of competition, since according to Greenfield, “any newcomer was regarded as a potential rival and there was smug satisfaction in seeing peers falter.” Although some competition can be a good thing, too much competition can lead to wasted resources, knowledge hoarding, and lack of cooperation. Eventually, problems go unaddressed because leaders lack the information and perspective necessary to overcome them.
Lehmann Brothers had a strong belief in the firm as a family. While this is generally a positive attribute – with, for example, the firm rushing to help when an employee had an ill family member – too much of a family culture means that the hierarchy is rigid and unyielding in decision making. When the firm had 8,000 employees, having only a handful of people at the top making the key decisions may have worked, as these were the handful that Lehmann believed really understood the business. By the end of 2008, the firm had grown large and complex, but the hierarchical family decision-making structure had not changed. The executive committee briefly tried to expand its membership, involving more in the decision-making process, but this effort was short-lived and threatened those in power. The case of Lehman shows that when organizations fail to break down rigid hierarchies, learning and adaptation are the primary victims.
Lehman Brothers’ ultimate bankruptcy stands in sharp contrast to the organizational learning demonstrated by hospitals that adopted the catheter safety procedures. The contrast cannot be overstated: Leaders who foster learning in organizations perform better, provide better work environments for employees, and stand a stronger chance of survival in the face of threats or challenges, as the next example confirms.
Learning-Directed Leadership in Consulting Firms
Whether the organization is involved in healthcare, professional services, or other fields, learning provides an advantage. A recent study by Richard Boyatzis (2006) of Case Western Reserve University illustrates how learning connects to revenue. The study involved a professional service firm with more than 3,000 partners worldwide. Professional service firms serve as a good proving ground for the advantage of learning because they typify the kinds of problems commonly faced by knowledge workers. Only partners and those who ranked at the top of the firm based on quality of client relationships, performance in growing the business, and strength in managing the practice were included. Thirty-two of the top-ranked performers met the benchmark as the best of the best. On average, the partners billed $2.4 million annually and produced a gross margin of 57 percent.
The study first gauged the behaviors and attitudes of the senior partners using a 360-degree feedback process, with five of the partners’ peers, five of their subordinates, and their boss completing a survey. Each partner also completed the survey. The survey sought feedback on 20 different competencies considered important by the organization. One cluster of competencies involved leadership, initiative, and planning. The second included knowledge-based competencies such as pattern recognition, systems thinking, and general knowledge of the job. A third cluster measured the degree to which senior partners valued learning and facilitated learning in others.
Just over a year and half later, the researchers looked at the relationship between the competencies and the partners’ performance. Performance was measured using two clear, agreed-upon measures: revenue, or how much money the partners brought into the firm, and gross margin, or how well the partner utilized the organization’s resources. Once the researchers collected this data, they then conducted various analyses on the relationship between these two performance measures and the 20 competencies.
The results resonate with learning-directed leadership. While several competencies showed value for performance, only two correlated significantly with both revenue and gross margin: valuing learning and facilitating learning in others. We estimate that the competency of valuing learning accounted for almost $800,000 in additional revenue. Facilitating learning accounted for an additional $1.6 million! Performance on gross margin was more than 10 percent higher for those senior partners who valued and facilitated learning.
As with any study, this one had limitations; however, it provides evidence of a clear relationship between desired performance outcomes and the value of learning-directed behaviors. The study not only shows the importance of learning in knowledge work, but also provides solid evidence of how important it is for leaders to facilitate learning in others.
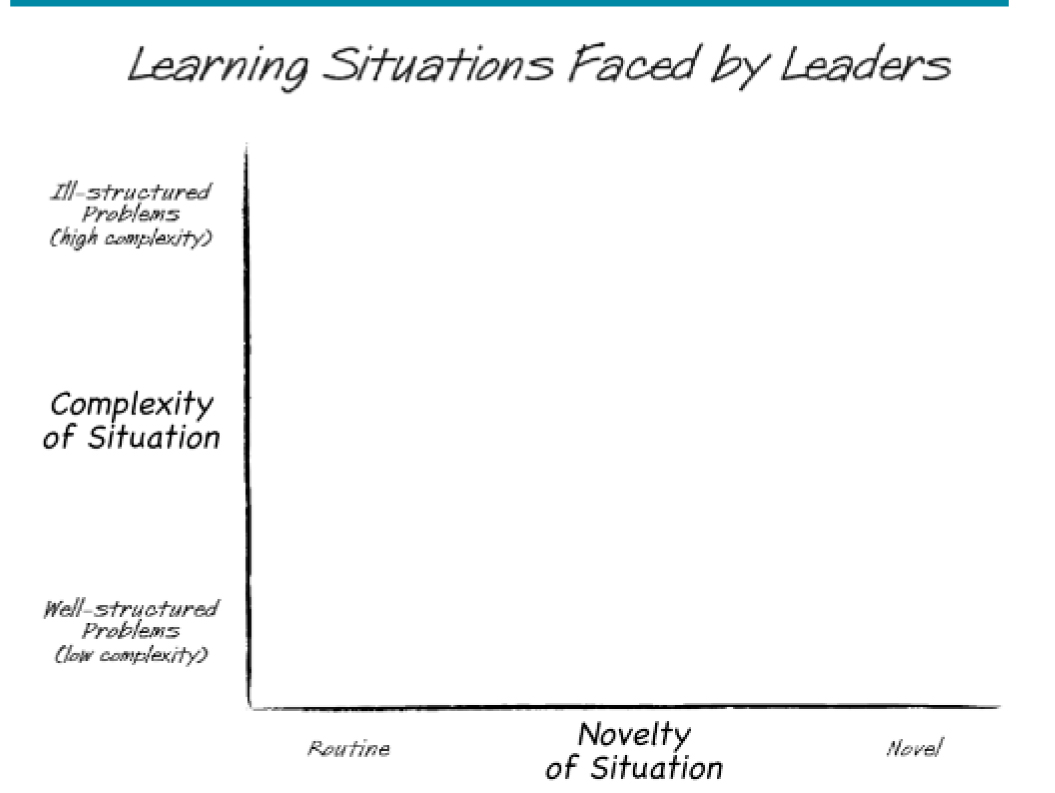
Identifying new problems faced by clients, forging new relationships, and building new business lie at the heart of consulting work. Recall the distinction between ill-structured and well-structured problems. A second consideration for learning involves learning in the face of both complexity and novelty. “Learning Situations Based on Complexity and Novelty” plots these considerations along two dimensions.
Leaders in the medical profession and consultants share something in common: learning in the face of complexity. For the medical professionals, the situation involved routine. The physicians involved in the effort to decrease catheter-related infections learned by focusing on the most important issues and standardizing procedures. The consultants, on the other hand, learned to identify novel situations and new business opportunities. The physicians and consultants both employed learning to improve organizational performance, but learned different things. Of course, the nature of learning is constantly shifting. The consultants will at some point need to learn under routine, just as the medical professionals will also face novel problems.
Conclusion
Through the examples above, we can begin to see how the demands of novelty and complexity shape leadership. The stories of learning in this article highlight the remarkable link between leadership, learning, and organizational performance. We provided examples of how expertise, knowledge, and creativity hold a clear advantage over position, influence, and authority. Ultimately, leadership is embedded in learning-directed actions.
LEARNING SITUATIONS BASED ON COMPLEXITY AND NOVELTY
© 2011 Anna B. Kayes and D. Christopher Kayes
Anna B. Kayes (EdD, the George Washington University) is Associate Professor of Business in the School of Business and Leadership at Stevenson University. She is author of articles on learning and leadership in outlets such as the Journal of Managerial Psychology and the Journal of Management Education, and is co-author of the forthcoming book, The Learning Advantage: The Six Practices of Learning Directed Leadership.
D. Christopher Kayes (PhD, Case Western Reserve University) is Dean’s Research Scholar and Associate Professor of Management at the George Washington University. His article, “The Destructive Pursuit of Idealized Goals,” was recognized as the most significant contribution to the practice of management by the Organizational Behavior Division of the Academy of Management. He is the author of “Destructive Goal Pursuit: The Mt. Everest Disaster” and co-author of the forthcoming The Learning Advantage: The Six Practices of Learning Directed Leadership.
References
American Management Association. How to build a high performance organization, 2007. [link]
Boyatzis, R. E., “Using tipping points of emotional intelligence and cognitive competencies to predict financial performance of leaders,” Psicothema, 18, 2006.
The Economist, “Data, data everywhere. A special report on managing information,” February 27, 2010).
Greenfield, H., “The decline of the best: An insider’s lessons from Lehman Brothers,” Leader to Leader, 55, 2010.
Landro, L., “Building team spirit: Nurses hesitate to challenge doctors even when doctors are ordering the wrong drug or operating on the wrong limb,” Wall Street Journal Online, February 16, 2010.
Mills, T. M. The Sociology of Small Groups. Prentice-Hall, 1967.
Patel, V. L., Groen, G. J., & Frederiksen, C. H., “Differences between students and physicians in memory for clinical cases,” Medical Education, 20, 1986.
Pronovost, P., &Vohr, E. Safe Patients, Smart Hospitals: How One Doctor’s Checklist Can Help Us Change Health Care from the Inside Out. Hudson Street Press, 2010.
Reason, J., “Safety in the operating theatre — Part 2: Human error and organizational failure,” Current Anesthesia and Critical Care, 6, 1995.
Wegner, T. G., & Wegner, D. M., “Transactive memory,” in A. S. R. Manstead & M. Hewstone (Eds.), The Blackwell Encyclopedia of Social Psychology, Blackwell, 1995.